Lumbar Radiculopathy (pinched spinal nerve, sciatica)
Lumbar radiculopathy refers to symptoms from irritation or compression of one or more of the nerve roots that arise from the spinal cord and then travel down to the legs. Symptoms may include pain that radiates down one or both legs or into the buttock or groin, weakness of leg muscles, a loss of sensation (numbness), and tingling in the buttock, leg, or foot. Severely affected patients may even have incontinence. Patients may have just one or any combination of the above symptoms.
The cause of lumbar radiculopathy is usually pinching/compression of a nerve near where it emerges from the spine in the low back. This can be due to a herniated disc or disc bulge, degenerative arthritis, infection, or other problems. Radiculopathy due to certain causes may improve or even resolve with time without the need for surgery (for example, a herniated disc). Symptoms due to other causes may not improve with time - even with medications and physical therapy. Surgery should be considered for patients with bothersome symptoms that have not resolved despite trials of non-surgical treatments, usually including physical therapy and a steroid injection.
For patients with persistent and bothersome symptoms from lumbar radiculopathy, surgery represents a definitive treatment option. Most patients who undergo surgery for lumbar radiculopathy can expect marked improvement or resolution of their leg symptoms, though some symptoms may take longer than others (for example, numbness tends to take longer to improve than pain). There are surgical options from the front, back, and side of the spine (i.e. "anterior,” "posterior," and “lateral”).
Posterior approaches are used most commonly for lumbar radiculopathy. Options include lumbar discectomy, and laminectomy, with or without lumbar fusion (e.g. TLIF, etc.). Anterior options include anterior lumbar interbody fusion (ALIF) and lumbar arthroplasty (disc replacement). Lateral options include oblique lumbar interbody fusion (OLIF). Each of these options has benefits and drawbacks.
For most cases of lumbar radiculopathy, I aim to avoid a fusion, if possible. The right option for you will depend on your symptoms, the number of spinal levels affected, and factors related to your medical history, smoking status, age, and spinal anatomy.
If you live near Denver and are suffering from lumbar radiculopathy, please consider meeting me in consultation to learn more about your treatment options.
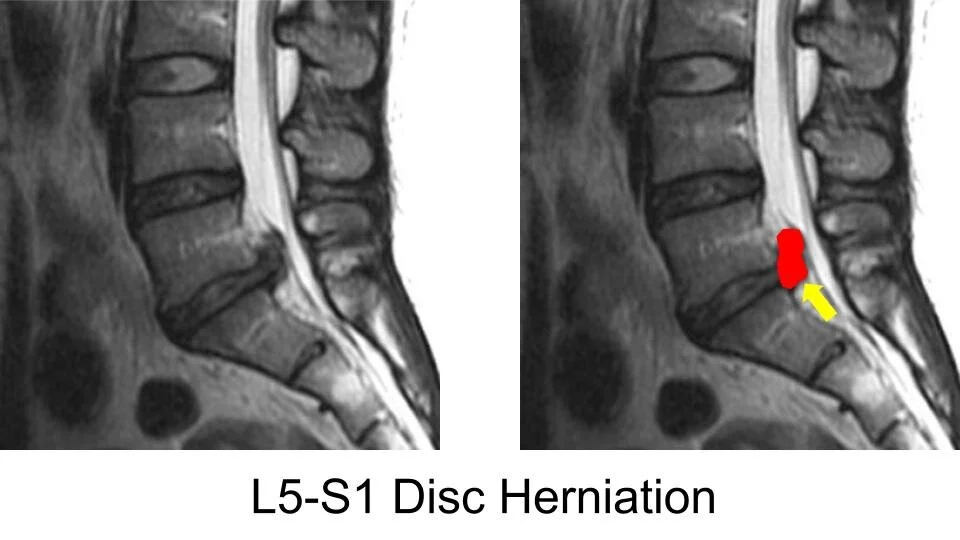
L5-S1 disc herniation causing S1 radiculopathy.