Essential Tremor
I have a particular interest and specialized training in caring for patients with movement disorders like Essential Tremor (ET), and I am the director of movement disorder surgery at Swedish Medical Center.
Below is additional information on ET. If you live near Denver and have ET, please consider meeting me in consultation to learn about treatment options.
Here is a link to an educational handout I provide patients who are considering surgery for ET. You can also visit my DBS patient guide and focused ultrasound patient guide.
-
Essential Tremor (ET) is a neurologic disorder that causes rhythmic shaking or trembling of one or more parts of the body. It is also referred to as benign tremor or familial tremor. ET is common, affecting roughly 10 million people in the United States.
In ET, the arms and hands are most commonly affected, but the legs, trunk, head, and voice can also be involved. The tremor tends to be most obvious when holding a posture with the arms outstretched or performing fine motor activities like eating, drinking, or writing.
ET can run in families, meaning that some patients have a parent, sibling, or child who is also affected. The symptoms tend to worsen slowly, but they can sometimes become disabling. ET can also cause social anxiety because the tremor is often noticeable in public and may lead to dropping items or spilling food or drink when eating out.
-
ET is usually diagnosed by a neurologist or a primary care doctor. Your doctor will ask questions about your tremor and also observe your tremor to distinguish it from other neurologic disorders. The diagnosis of ET is clinical, meaning that it is based on your symptoms and a physical exam by a doctor. There is as yet no X-ray, MRI, or blood test to diagnose ET, though your doctor may order these in certain cases to help rule out other problems.
Treatments for ET are aimed at reducing tremor symptoms, and they start with medications. Propranolol and primidone are the two most commonly used drugs. These can offer some patients substantial tremor relief. For patients who continue to have severe tremor symptoms despite medications, surgery is an option. There are two types of surgery for ET: deep brain stimulation (DBS) and thalamotomy. These are described in more detail below.
-
Surgery is worth considering when a patient has tried two or more medicines for tremor and continues to experience symptoms that are disruptive to their daily life or when the medications cannot be tolerated due to side effects.
-
Deep brain stimulation (DBS) has been used for over 20 years in the United States for patients with medication-resistant ET. In a DBS procedure, a neurosurgeon introduces a thin wire into the brain. The wire is connected to a pacemaker that is inserted beneath the skin under the collarbone. The pacemaker delivers painless electrical pulses to the brain. DBS provides long-lasting tremor suppression. The results can be dramatic, and there are countless videos online showcasing its effects (one example here). DBS is reversible and also flexible, meaning the therapy can be adjusted as a patient’s symptoms change over time.
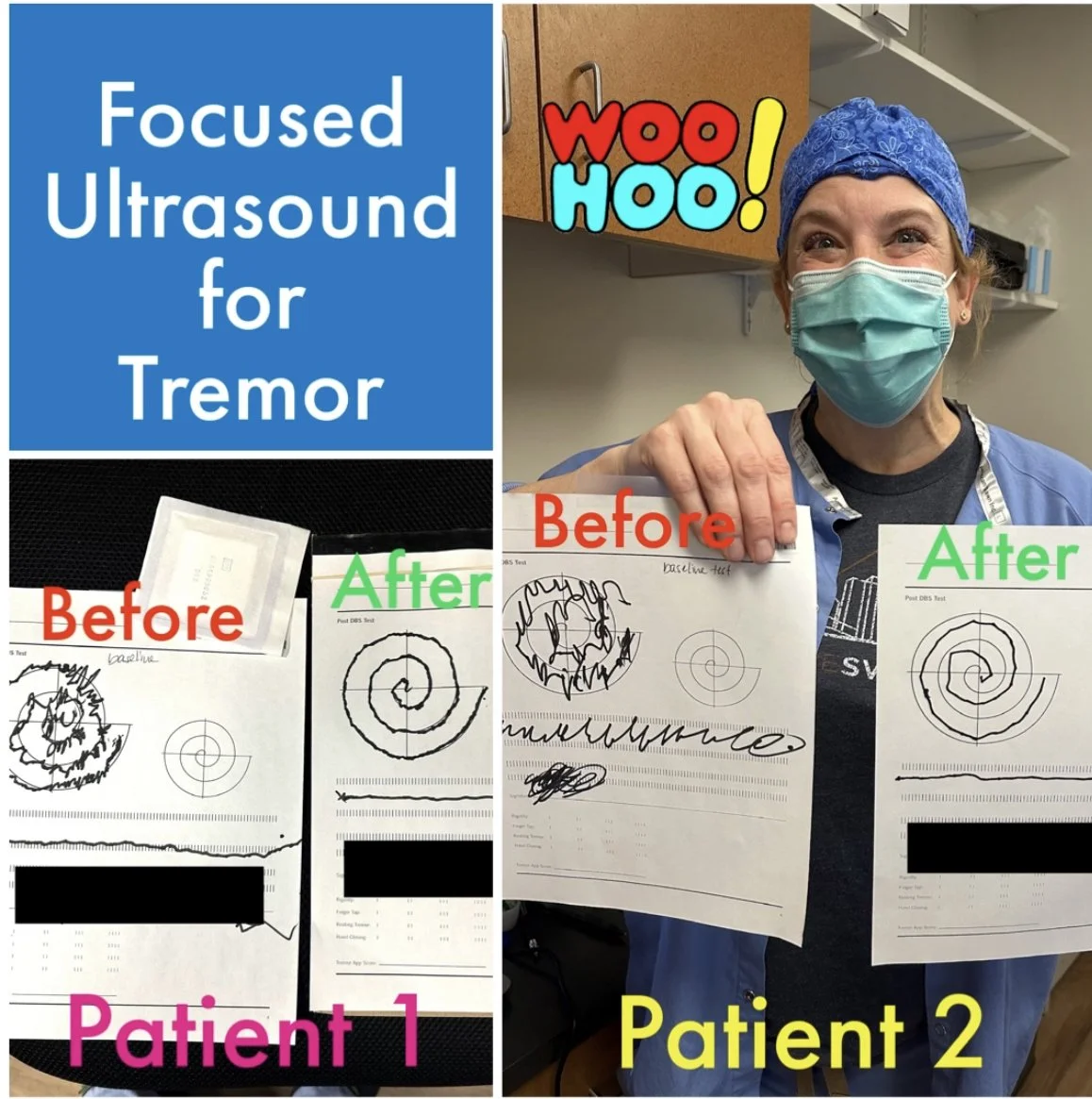
Thalamotomy is a second surgical option for ET. It involves creating a small lesion in the brain to disrupt a neural circuit involved in tremor. Thalamotomy procedures have the advantage of not requiring a medical implant. There are three methods for performing thalamotmy: MRI-guided focused ultrasound, Gamma Knife, and radiofrequency.
-
Surgical candidates should have bothersome tremor despite trials of two or more tremor medications. Tremor affecting the hands tends to respond the best to surgery. Head and voice tremor are more variable in their response to treatment.
-
For those with hand tremor who have DBS surgery, 85-90% of patients experience a reduction in their tremor severity by 90% or more. This means that most patients see a very significant reduction in tremor. DBS is not a cure, however, so the tremor may not disappear completely. The effects of DBS last for years, and DBS therapy can be turned up or down as your symptoms change over time.
-
First, please request a referral from the doctor who treats your ET. I prefer a doctor referral over a self-referral because a referral from your doctor will include records of your tremor care.
Second, please review the following questions before our visit:
* When did your tremor begin, and where in the body did it start?
* Which parts of your body are most affected now?
* What kinds of movements bring out your tremor?
* Which important activities in your daily life are most affected by your tremor?
* Which medications have you tried, and which ones helped?
* Does tremor run in your family?
* Does anything make your tremor better or worse (including alcohol)?
* Have you noticed any other problems with movement besides your tremor?
-
Once again, for patients considering DBS surgery, you can visit my DBS Patient Guide to learn more about what to expect during the process. If you are considering focused ultrasound, I have a similar patient guide here.
You can also read more about the surgical robot that I use to help make DBS surgery more efficient, accurate, and safe and the incision-less techniques I use to perform thalamotomy.

If you or a family member is affected by essential tremor, please consider meeting me in consultation to learn more about your treatment options.